Computer Navigation is for the Outliers!!!!!!
- By Dr Kaushik Hazratwala, Orthopaedic Surgeon,
- Director – Orthopaedic Research Institute of Qld
- Director – Townsville Lower Limb Clinic
Finally, after 15 yrs. this Korean group has proven that Computer Navigation will not improve patient outcome in all comers. The proponents of conventional Knee replacements will rejoice in this publication and uncork expensive French champagne. Finally, their resistance to adopting Computer navigation has been vilified.
So why do we still have a 20% dissatisfaction rate in patient following a “successful” TKR. Is it because some surgeons are poor technicians and are diluting the data for the super gifted surgeon. Or is it that 20% of the population undergoing TKR are just whingers. Could it be that we as surgeons are not catering for that 20%? God forbid it’s the later!!!!!!!
Let’s look at some published data on anatomical variation amongst the normal population. Belleman's et al1 in 2013 found that approximately 20% of the population is outside the +/- 3° Hip Knee Ankle Alignment (HKA). These are asymptomatic patients whose knees are not Straight. Below is a graph form this paper demonstrating the spread of constitutional alignment.
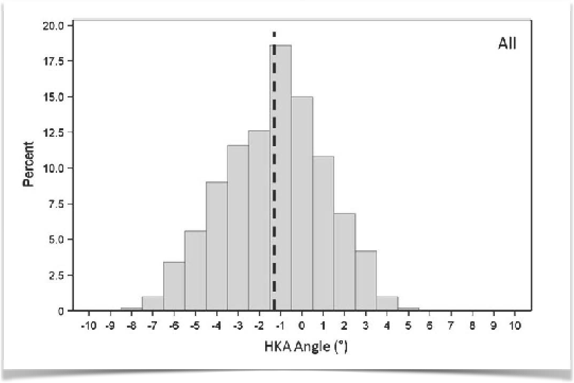
Fig 1- 24.6% of the sampled population had a constitutional Varus of greater than 3° Varus, and 2.4% were greater than 3° valgus.
So why do we aim to align our knees to within +/-3°? The answer lies in the fact that we cannot accurately vary the degree of resection within 1° of accuracy with conventional instruments. The margin of error that has led to older publication 2345 agreeing with the fact that knees have a higher failure rate if outside the 3° window of safety. Some of these studies included poorly designed prosthesis and notwithstanding the fact that these knees were implanted using the mechanical alignment technique and the fact they ended up outside the 3° widow was an error. These knees were then followed up to show inferior results and a higher failure rate. Hardly surprising!!
Conventional technique works great for the 80% of the population utilizing the mechanical alignment technique and subsequent soft tissue release to balance the knee. If the same surgical technique is used using computer navigation one would have to be foolish to expect a different outcome. All the computer navigation does is help the surgeon hit the target +/-3° more precisely. Many papers have shown the superiority of CAS over conventional instruments678. Deep et el7 have performed a metaanalysis on this topic and found that the current literature does support the use of CAS and in the future assistive technologies will pave the way for superior outcomes.
I’m proposing a shift in the way we look at Knee replacement assistive technology. We currently have 3 basic forms of assistive technology, CAS, IDI (Image derived instrumentation) and Robotics. These technologies are not a prescription to perform a knee replacement but rather a guide and a tool to execute your pre-operative plan.
If you are able to predict the outliers and tailor your surgery to realign not only the bony anatomy but also restore the soft tissue envelope to its native alignment I would think that we might just see better outcomes. This change in mindset could lead to the drop in the 20% dissatisfaction rate.
I have no issue with the conventional instruments as long as the surgical algorithm allows the surgeon to vary the resection angle to the pre-operative templated angles. I have been thru this curve and have settled on navigation as the gold standard in the execution of a plan that is not necessarily +/-3°. Our research group (Orthopaedic Research Institute of Queensland) is currently looking at outcome data of bilateral patients who are constitutional outliers and have been either mechanically or alternately aligned. Both groups have been done using the CAS. The Game is not within +/-3° it is outside this range. The 80% good results in both groups dilute the 20% outlier poor result in the machine when compared to the alternately aligned outliers.
Therefore, let’s not rejoice in this paper – let’s be critical and let’s work towards dropping the dissatisfaction rate to whatever we can.
- Bellemans J, Colyn W, Vandenneucker H, Victor J. The Chitranjan Ranawat award: is neutral mechanical alignment normal for all patients? The concept of constitutional varus. Clin Orthop Relat Res. 2012;470(1):45-53. doi:10.1007/s11999-011-1936-5.
- Bonner TJ, Eardley WGP, Patterson P, Gregg PJ. The effect of postoperative mechanical axis alignment on the survival of primary total knee replacements after a follow-up of 15 years. J Bone Jt Surg Br. 2011;9393(9):1217-1222. doi:10.1302/0301-620X.93B9.
- Eckhoff DG, Bach JM, Spitzer VM, et al. Three-dimensional mechanics, kinematics, and morphology of the knee viewed in virtual reality. J Bone Joint Surg Am. 2005;87 Suppl 2(suppl_2):71-80. doi:10.2106/JBJS.E.00440.
- Parratte S, Pagnano MW, Trousdale RT, Berry DJ. Effect of postoperative mechanical axis alignment on the fifteen-year survival of modern, cemented total knee replacements. J Bone Joint Surg Am. 2010;92(12):2143-2149. doi:10.2106/JBJS.J.00937.
- Lotke PA, Ecker ML. Influence of positioning of the prosthesis in total knee replacement. J Bone Joint Surg Am. 1977;59(1):77-79. http://www.ncbi.nlm.nih.gov/pubmed/833180. Accessed January 27, 2018.
- Todesca A, Garro L, Penna M, Bejui-Hugues J. Conventional versus computer-navigated TKA: a prospective randomized study. Knee Surgery, Sport Traumatol Arthrosc. 2017;25(6):1778-1783. doi:10.1007/s00167-016-4196-9.
- Deep K, Shankar S, Mahendra A. Computer assisted navigation in total knee and hip arthroplasty. doi:10.1051/sicotj/2017034.
- de Steiger RN, Liu Y-L, Graves SE. Computer Navigation for Total Knee Arthroplasty Reduces Revision Rate for Patients Less Than Sixty-five Years of Age. J Bone Jt Surgery-American Vol. 2015;97(8):635-642. doi:10.2106/JBJS.M.01496.